Background
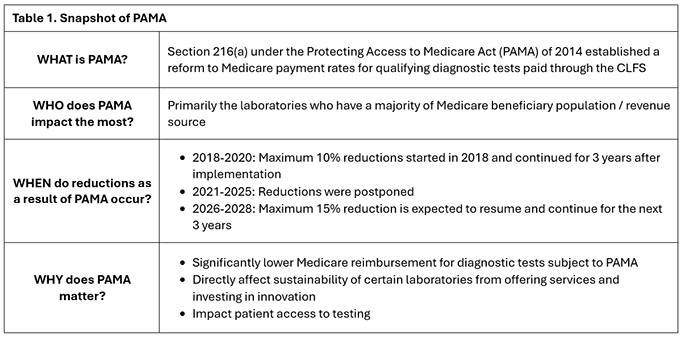
The Clinical Laboratory Fee Schedule (CLFS) is Medicare’s payment system for clinical laboratory diagnostic tests described by either Category I CPT codes or proprietary laboratory analyses (PLA) codes. While the reimbursement rates established on the CLFS were intended to be implemented nationally, inconsistencies in how they were applied and the lack of regular updates led to an increasing disparity between Medicare and private payer reimbursement rates. To help address this growing misalignment, Congress passed the Protecting Access to Medicare Act (PAMA) in 2014, which reformed how Medicare payment rates for qualifying laboratory tests listed on the CLFS were calculated, with the goal of aligning Medicare payment rates with private payer reimbursement.
Because Medicare historically paid more than private payers for most laboratory tests, the recalculated CLFS Medicare rates for tests subject to PAMA were expected to be significantly reduced. To mitigate the impact on laboratories, PAMA payment reductions were set to be phased in over a 6-year period. For the first three years, the annual payment reduction would be capped at 10%, and at 15% for the remaining three years.
The initial payment reductions of up to 10% went into effect on January 1, 2018, for applicable CLFS listed test codes, and were followed by additional 10% reductions on January 1, 2019, and January 1, 2020. Payment reductions under PAMA were delayed from 2021 to 2025 but are scheduled to resume on January 31, 2026. With the impending resumption, PAMA reductions will increase to a maximum of 15% in January 2026, January 2027, and January 2028.
The initial 2018 PAMA-adjusted Medicare CLFS payment amounts were determined by the weighted median of private payer rates and test volumes reported to CMS in 2016 by ‘applicable laboratories’, meaning the laboratory:
- Bills Medicare Part B under its own National Provider Identifier (NPI) or bills on Form CMS-1450 under type of bill (TOB) 14x; and
- Has a combined revenue from the Medicare CLFS and Physician Fee Schedule (PFS) that constitutes over 50% of their total Medicare revenue; and
- Receives at least $12,500 of its Medicare revenue from the CLFS during the data collection period.
However, the 2016 data collection and reporting period inadvertently favored large national reference laboratories that often accept lower reimbursement rates and prioritize volume-based contracts. This skewed the data, resulting in larger-than-expected payment reductions on routine tests. The greatest impact was felt by hospital and smaller independent laboratories that typically have lower volumes, but rely on test revenue to sustain them, whereas larger reference laboratories are more equipped to absorb the reductions due to their large volume of testing.
Implications of PAMA on Routine & Innovative Testing
The impact of PAMA is evident across the entire CLFS, affecting both routine laboratory tests described by Category I CPT codes and innovative, novel assays described by PLA codes. For example, routine diagnostic tests such as complete blood count and basic metabolic panel typically receive low reimbursement from commercial payers because they are performed under high-volume contracts; under PAMA, these lower private payer prices translate into the maximum 10% reduction to Medicare reimbursement for the affected codes.
For manufacturers / laboratories launching innovative diagnostics, PAMA has introduced added complexity, requiring a comprehensive understanding of how different strategic coding approaches affect payment assignment and the pricing potential of their new test.
- Scenario #1 Utilizing Existing Category I CPT Code: If a laboratory bills for a test using an existing Category I CPT code with a broad descriptor that can be used to describe many different tests, the combined volume and revenue for all tests billed under that code may cause the laboratory to meet PAMA reporting thresholds. In this scenario, every test billed under that Category I CPT code, regardless of the laboratory where the test is performed, could face payment reductions, even if a specific test using the Category I CPT code has low commercial volume.
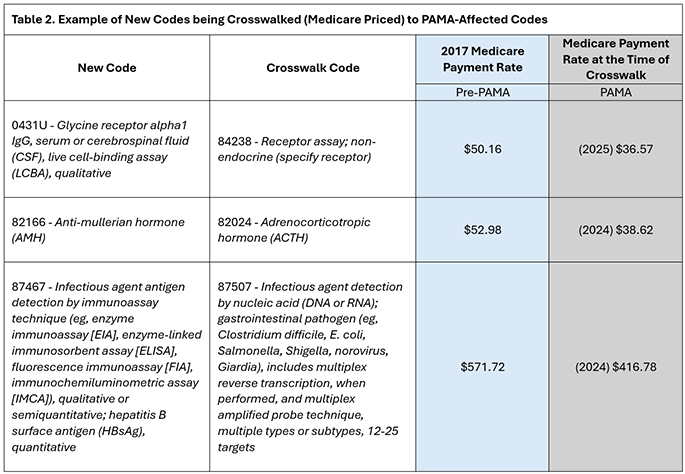
- Scenario #2 Seeking a Novel Code: To mitigate future payment reductions under PAMA and establish assay-specific pricing, manufacturers and/or laboratories can consider seeking a new code, Category I CPT or PLA, to describe their test. After a new code is granted, Medicare rate setting is determined through either crosswalk, assigning payment based on similarities to existing tests listed on the CLFS, or gapfill, a bottom-up calculation of test costs and associated resources. When a new test is priced through crosswalk, its initial Medicare rate may be influenced by PAMA if the crosswalked code has already experienced PAMA payment reductions. In this scenario, the new test inherits the reduced payment rate (see Table 2 for examples). While the new code adopts the parent code’s reduced rate at the time of crosswalk, it is not subject to additional PAMA reductions that may apply to the parent code in the subsequent years.
PAMA in 2026
PAMA data reporting and payment rate cuts of up to 15% are set to resume on January 31, 2026, unless Congress intervenes to delay them or enact new reforms to prevent impending and future cuts.
A key piece of legislation that the laboratory industry is closely monitoring as it may impact the reinstatement of PAMA payment reductions, is the Reforming and Enhancing Sustainable Updates to Laboratory Testing Services (RESULTS) Act. The RESULTS Act was introduced in September 2025 as bipartisan legislation to protect Medicare beneficiaries’ access to laboratory testing and reform PAMA by improving the CLFS rate-setting process. The RESULTS Act, if passed in both houses of Congress and signed into law, would enhance the accuracy of data used to determine CLFS rates under PAMA, while reducing the administrative burden associated with CMS reporting. The RESULTS Act has not yet become law.
By reducing overall laboratory revenue, payment cuts under PAMA may influence manufacturers and/or laboratories’ decisions to launch new tests, invest in advanced technologies, and ensure patient access to innovative diagnostics.
Are you prepared for the return of PAMA in 2026? BeaconOne Healthcare Partners can help you develop a strategic US market access plan that optimizes pricing, navigate evidence and timeline considerations, and positions your test for long-term success.
BeaconOne is actively tracking and engaging in the evolving US and O-US policy and reimbursement landscape for laboratory services. Contact us to learn more about our capabilities.